 膜杰作
膜杰作 Star Staining
Star Staining







抗体来源(Source)
Anti-Bevacizumab Antibody (AY10) is a Mouse monoclonal antibody produced from a hybridoma created by fusing SP2/0 myeloma and Mouse B-lymphocytes.
克隆号(Clone)
AY10
种属(Species)
Mouse
亚型(Isotype)
Mouse IgG1/kappa
抗体类型(Antibody Type)
Hybridoma Monoclonal
种属反应性(Reactivity)
Human
免疫原(Immunogen)
Bevacizumab.
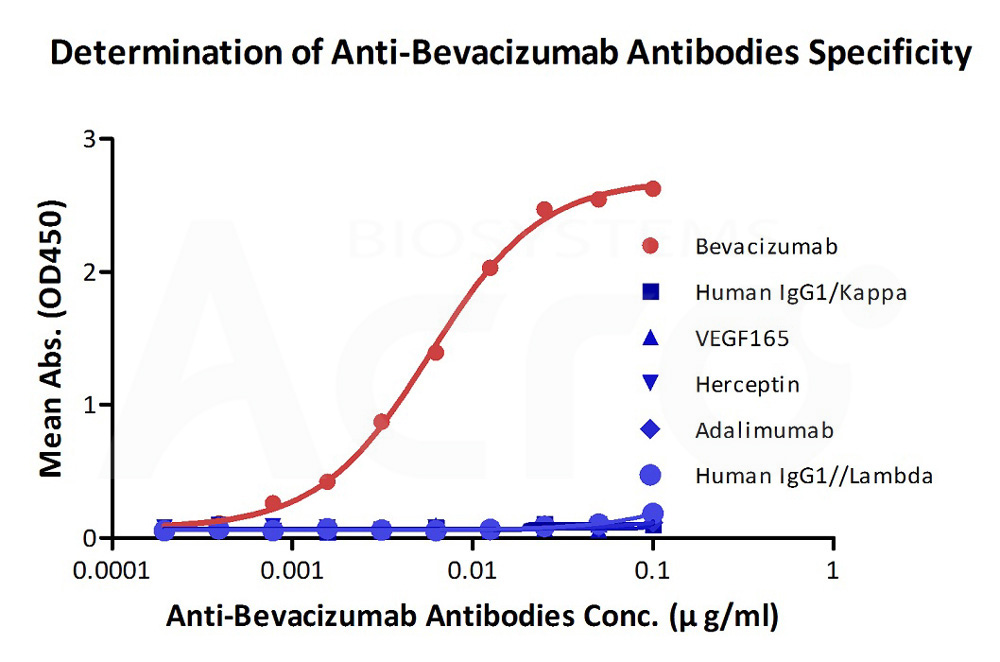
特异性(Specificity)
Recognizes Bevacizumab specifically.
应用(Application)
| Application | Recommended Usage |
| ELISA | 10-20000 ng/mL |
纯度(Purity)
>95% as determined by SDS-PAGE.
>95% as determined by SEC-MALS.
纯化(Purification)
Protein A purified / Protein G purified
制剂(Formulation)
Lyophilized from 0.22 μm filtered solution in Tris with Glycine, Arginine and NaCl, pH7.5 with trehalose as protectant.
Contact us for customized product form or formulation.
重构方法(Reconstitution)
Please see Certificate of Analysis for specific instructions.
For best performance, we strongly recommend you to follow the reconstitution protocol provided in the CoA.
存储(Storage)
For long term storage, the product should be stored at lyophilized state at -20°C or lower.
Please avoid repeated freeze-thaw cycles.
This product is stable after storage at:
- 4-8°C for 12 months in lyophilized state;
- -70°C for 12 months under sterile conditions after reconstitution.
质量管理控制体系(QMS)
电泳(SDS-PAGE)
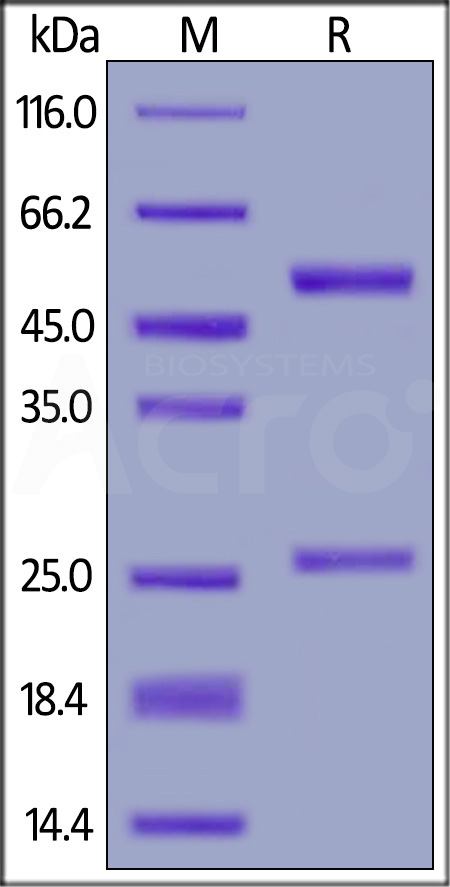
Anti-Bevacizumab Antibody (AY10) on SDS-PAGE under reducing (R) condition. The gel was stained with Coomassie Blue. The purity of the protein is greater than 95%.
SEC-MALS
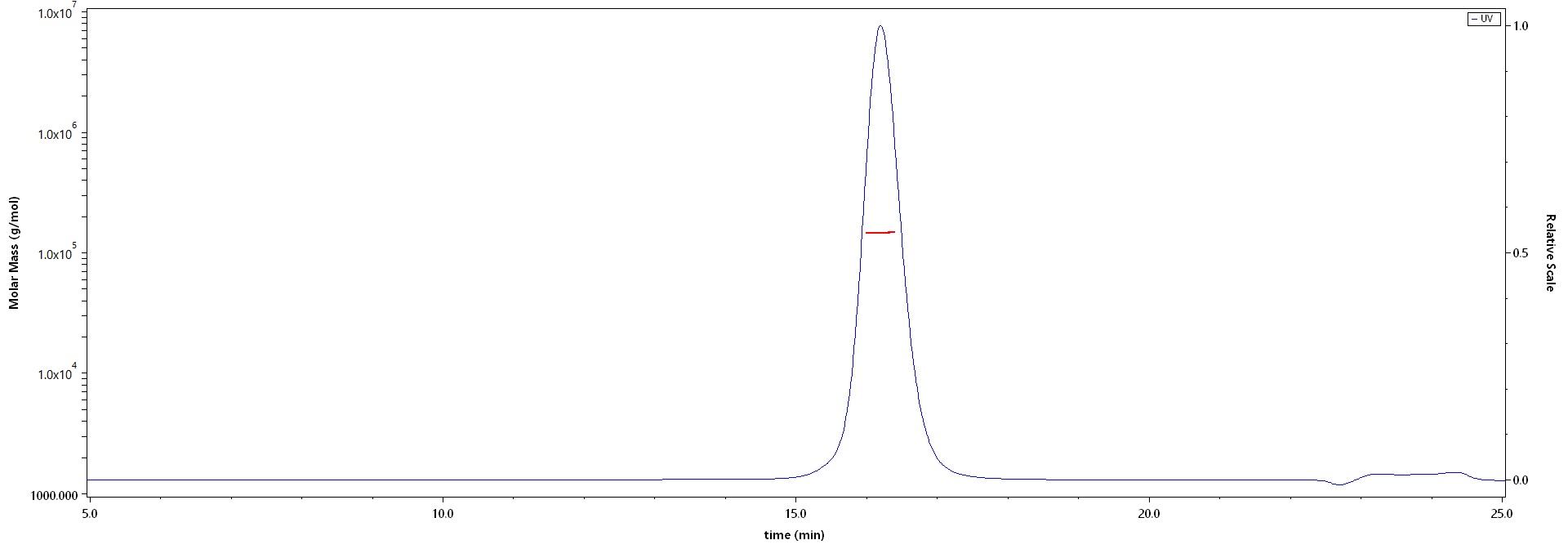
The purity of Anti-Bevacizumab Antibody (AY10) (Cat. No. BEB-Y10) is more than 95% and the molecular weight of this protein is around 135-155 kDa verified by SEC-MALS.
Report
活性(Bioactivity)-ELISA
Detection of bevacizumab by bridging ELISA in serum. Immobilized Anti-Bevacizumab Antibody (AY10) (Cat. No. BEB-Y10) at 2 μg/mL, add increasing concentrations of bevacizumab (10% human serum) and then add Biotinylated Anti-Bevacizumab Antibody (AY13) (Cat. No. BEB-BY13) at 2 μg/mL. Detection was performed using HRP-conjugated streptavidin with a sensitivity of 0.4 μg/mL (QC tested).
Protocol
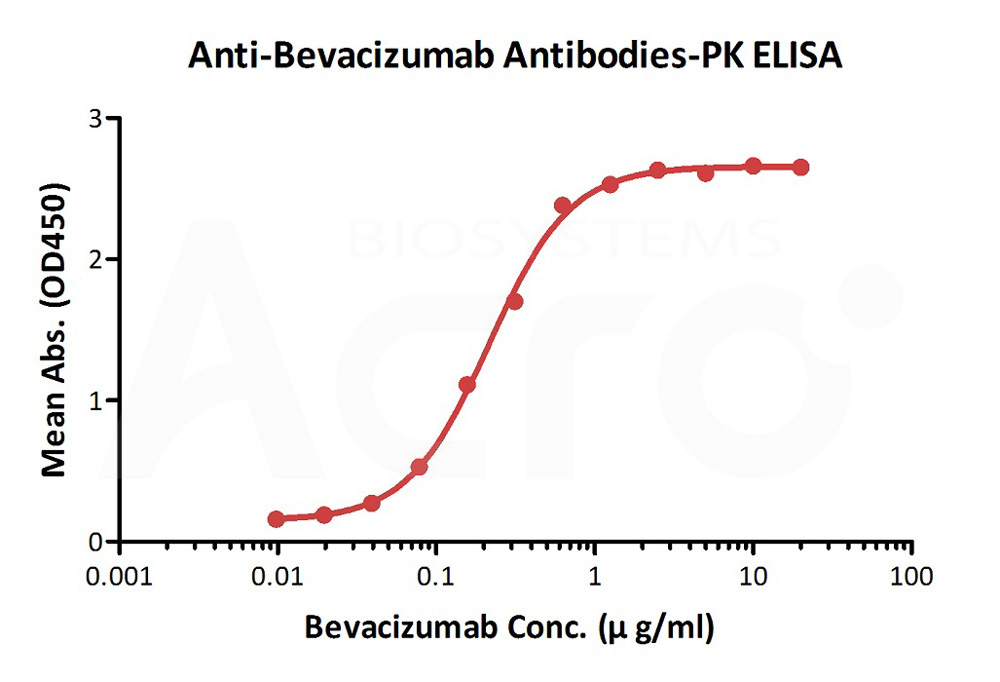
Immobilized Bevacizumab at 1 μg/mL (100 μL/well) can bind Anti-Bevacizumab Antibody (AY10) (Cat. No. BEB-Y10) with a linear range of 0.39-25 ng/mL.
Protocol
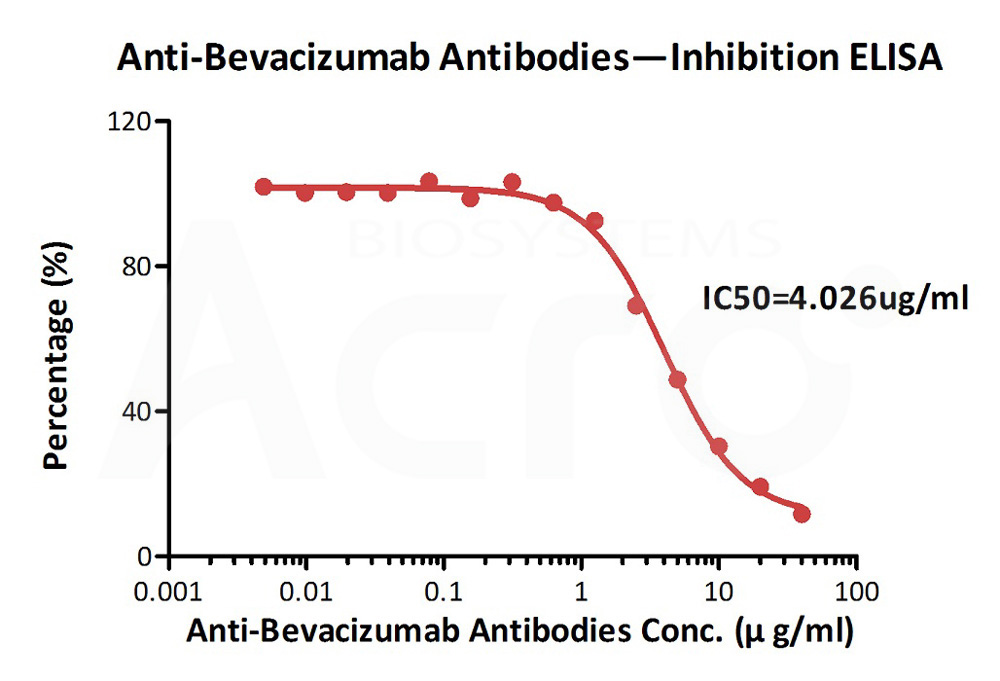
Immobilized Bevacizumab at 2 μg/mL (100 μL/well) can bind pre-mixed Anti-Bevacizumab Antibody (AY10) (Cat. No. BEB-Y10) and Biotinylated Human VEGF165, His,Avitag (Cat. No. VE5-H82Q0) with a inhibition rate of 81%.
Protocol


产品推荐(Recommended Products)

背景(Background)
A recombinant humanized monoclonal IgG1 antibody that binds to and inhibits the biologic activity of human vascular endothelial growth factor (VEGF). Bevacizumab contains human framework regions and the complementarity-determining regions of a murine antibody that binds to VEGF. Bevacizumab is produced in a Chinese Hamster Ovary mammalian cell expression system in a nutrient medium containing the antibiotic gentamicin and has a molecular weight of approximately 149 kilodaltons.